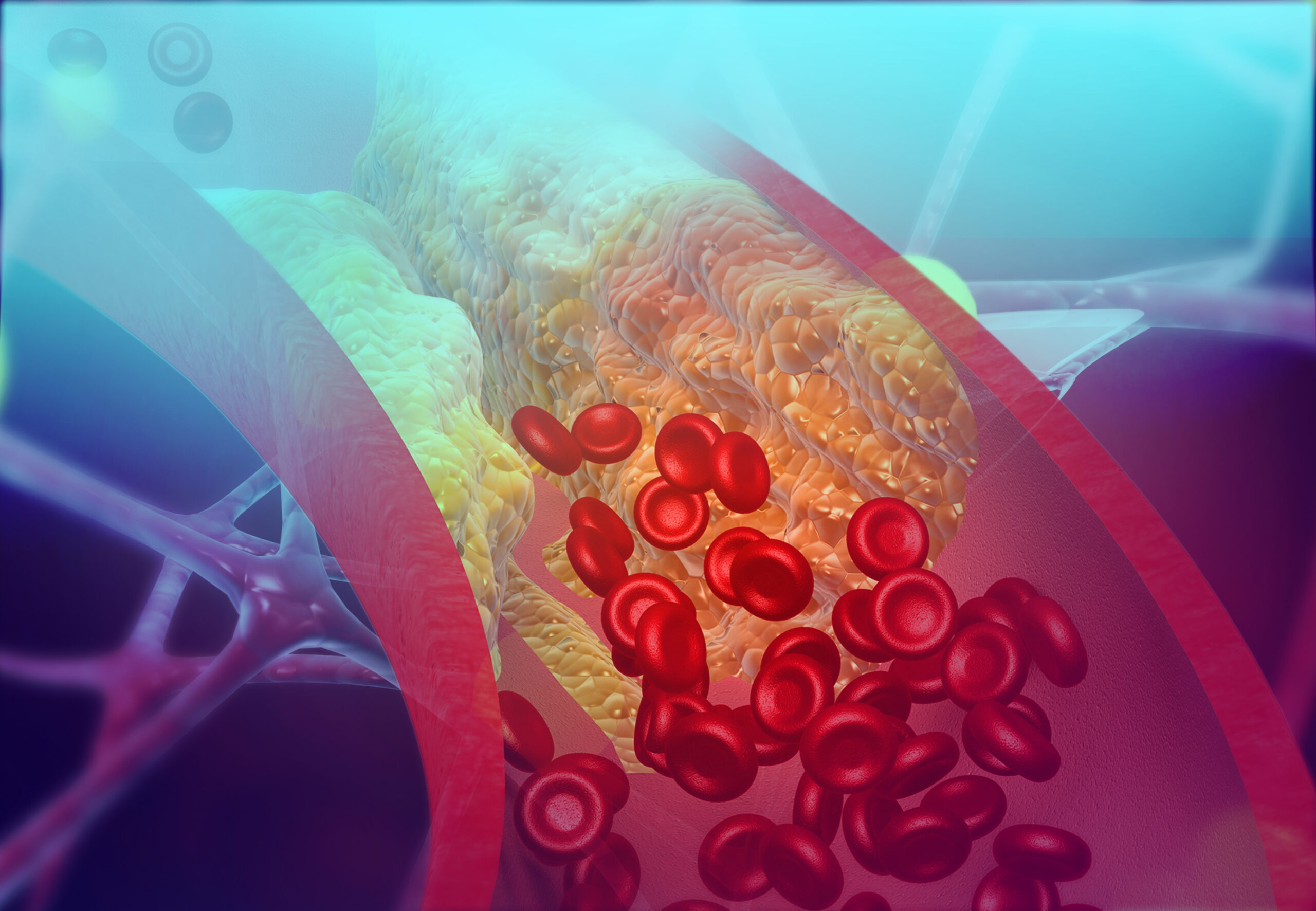

Before there was widespread use of statins to lower blood cholesterol, before the medical community found better strategies for treating high blood pressure, and before the public understood the cardiovascular benefits of eating less saturated fat and engaging in more physical activity, aspirin s...